BPP-what?
Time to stop the room from spinning (~5 min read)

Dizziness
is a common complaint among the general population and can have many underlying
causes but typically results as a disruption in the visual, somatosensory
or vestibular system. Up to 42% of patients with complaints of dizziness or
vertigo end up with the diagnosis of Benign Paroxysmal Positional Vertigo- or
BPPV.(1) This is one of the most common issues with our inner ear and is
defined as a disorder characterized by repeated episodes of positional vertigo.
While the name sounds intimidating, the good news is BPPV is one of the easiest vestibular conditions to treat which is critical because quality of life can be significantly impacted when living with BPPV. Patients with BPPV are at increased risk for falls, experience impairment in performance of daily activities and may have associated episodes of nausea.(2)
Breaking it down:
- Benign suggests that this is a non-life threatening condition of the central nervous system with a good prognosis- if left untreated 50% of individuals will have complete resolution of symptoms within 3 months, however with treatment it can resolve much faster.(2)
- Paroxysmal means that the symptoms are not constant but rather they rapidly or suddenly occur
- Positional suggests symptoms occur or are triggered by various movements of the head, and
- Vertigo means individuals experience the sensation of “ spinning ” or motion, either they are spinning or that the room is spinning around them.
Relationship of ear anatomy to BPPV
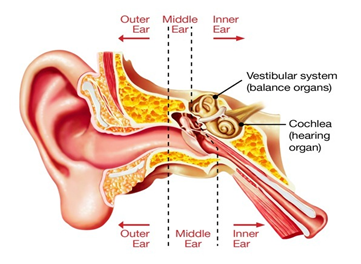
To fully understand the underlying mechanisms of BPPV it is essential to have a basic understanding of the anatomy of the ear. The outer ear, funnels sound vibrations from the external environment down the ear canal to the ear drum. Sound crosses the eardrum entering the middle ear, where it is conducted by 3 tiny bones called the malleus, incus and stapes to the inner ear (Figure 1).
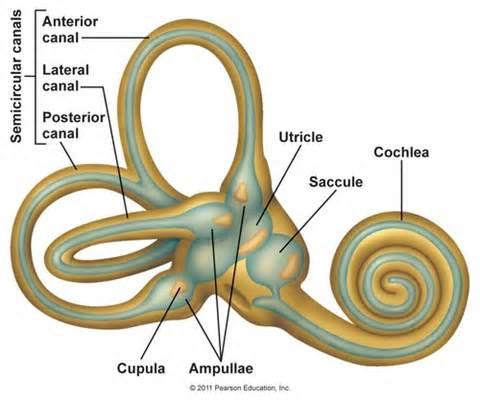
The inner ear is where the magic happens and is divided into two parts, sound information is processed in the cochlea and transmitted to the brain via the cochlear nerve which is how we recognize and interpret “sound.” The other part of the inner ear is the vestibular system (Figure 2), which consists of a complex bony labyrinth with 3 semicircular canals that are filled with fluid and each situated in a plane in which our head moves. The 3 semicircular canals (anterior, posterior and horizontal) respond to angular acceleration of the head (think shaking your head yes (vertical) or no (horizontal)) and the various orientations at 90 degrees to each other help us detect different directions of movement. When we move or change position, the fluid is displaced within the canals, flows into an expansion of the canal termed the ampulla and stimulates specialized hair cells in the cupulla to send feedback to the vestibular nerve to tell our brain which direction our head is moving. This signaling is essential to our ability to maintain balance and coordinate head and eye movements.
The vestibular system uses two other organs termed the otolith organs , which detect and respond to linear acceleration of the head and are sensitive to gravity. There are two otolith organs, the utricle which detects movement in the horizontal plane (think driving in a car), and the saccule which detects movement in the vertical plane (think riding in an elevator). Within the utricle and saccule there is a gelatinous membrane where calcium carbonate crystals called otoconia sit. The otoconia shift in response linear acceleration leading to movement in the layers of membrane below the otoconia and displacement of hair cells to again signal to our brain in which capacity our head is moving. If you’re feeling confused about the anatomy of the ear and have some free time check out this video for a moderately entertaining and more in depth explanation.
So, you’re telling me there are crystals in my ear? Yes,
that is correct! And these crystals are the leading culprit in symptoms of
vertigo. BPPV results when the crystals are dislodged from the gelatinous
membrane that they sit on in the otolith organs, and get misplaced into one of
the semicircular canals. This may occur without any mechanism of injury but can
also occur following trauma to the head. When the crystals are floating in the
canals where they do not belong, they disrupt the movement of fluid which changes
the firing rate of the hair cells and triggers the rapid onset of vertigo. Specific
to BPPV the actual “spinning” sensation is only temporary (most commonly a few
seconds to 1 minute) because when the crystals float and settle down on the
bottom of the canal the sensation stops—however, when you go to move your head
again the crystals are again floating in the canal and the symptoms will
resume.
How do I fix BPPV?
The most common occurrence of BPPV is canalithiasis, with crystals displaced into the posterior semicircular canal 85% of the time.(5) Physical Therapists will examine the presence and direction of abnormal eye movements while the patient is in a symptom provoking position, to determine which canal the crystals are displaced (posterior, anterior or horizontal), which ear is effected (left, right or both) and what type of BPPV is occurring (canalithiasis vs. cupulolithiasis). It is essential to have an appropriate diagnosis initially to determine treatment moving forward, therefore, despite a plethora of information on the internet, it is recommended to see a physical therapist trained in vestibular rehab.
There are 3 maneuvers to test for BPPV, the dix-hallpike test or the side-lying test (for those without cervical ROM to perform dix-hallpike or who cannot lie on their back) for the posterior canal.(6) To test the horizontal canal therapists will use the roll test.(7) These maneuvers may be completed with frenzel lenses or infrared lenses to maximally visualize eye movements. The direction of torsion within the eye is indicative of which canal the crystals have been displaced. Once it has been determined which canal the otoconia are dislodged, there are various canalith repositioning maneuvers for treatment to return the crystals back to where they belong and ultimately reduce symptoms.
Who can help me?
If you or someone that you know may be experiencing BPPV then schedule an initial evaluation with one of the therapists at Evolution Sports for thorough and individualized care to return you to your prior level of function!
References
- Bhattacharyya, N., Gubbels, S., Schwwartz, S., Edlow, J., El-Kashlan, H., Fife, T., et al. Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update). Otolaryngology Head and Neck Surgery . 2017:156:S1-S47.
- Lopez-Escamez JA, Gamiz MJ, Fernandez-Perez A, et al. Long-term outcome and health-related quality of life in benign paroxysmal positional vertigo. Eur Arch Otorhinolaryngol . 2005; 262: 507-511.
- Burton MJ, Eby TL, Rosenfeld RM. Extracts from the Cochrane Library: modifications of the Epley (canalith repositioning) maneuver for posterior canal benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg . 2012;147:407-411.
- von Brevern M, Bertholon P, Brandt T, et al. Benign paroxysmal positional vertigo: diagnostic criteria. J Vestib Res . 2015;25:105- 117.
- Parnes LS, Agrawal SK, Atlas J. Diagnosis and manage- ment of benign paroxysmal positional vertigo (BPPV). CMAJ . 2003;169:681-693.
- Viirre E, Purcell I, Baloh RW. The Dix-Hallpike test and the canalith repositioning maneuver. Laryngoscope . 2005;115:184-187.
- Casani AP, Nacci A, Dallan I, et al. Horizontal semicircular canal benign paroxysmal positional vertigo: effectiveness of two different methods of treatment. Audiol Neurootol . 2011;16:175-184